hypokinetic disease
disease associated with physical inactivity
habitual physical activity
what we do everyday, moving to get through the day
exercise
intentional physical activity to improve physical fitness
Sport fitness
Skilled base
Physical fitness
Everyday life
Types of PHYSICAL FITNESS:
HEALTH RELATED COMPONENTS:
-Cardiovascular fitness
-muscular strength
-muscular endurance
-flexibility
-body composition
SKILL-RELATED FITNESS COMPONENTS:
- Agility
- Balance
- Coordination
- Speed
-Power
-Reaction Time
Define hypokinetic disease (be sure to be able to give examples!)
A disease caused by physical inactivity
types of hypokinetic diseases:
-> Cardiovascular disease (CVD)
-> obesity
->Type 2 diabetes
->Osteoporosis
-> Mental ill-health
-> some types of cancer
Coronary heart disease
when coronary arteries are clogged with plaque caused by Atherosclerosis
Stroke
a blood clot in a vessel of the brain, blocks blood and O2 getting to areas of the brain, leading to tissue death
Hypertension
High blood pressure (140/90)
Obesity
Excess of body fat
Type 2 diabetes
Body becomes resistant to insulin produced by the pancreas (best treatment is exercise)
Osteoporosis
Low bone density, its like having holes in the bone, it makes it easier to break (to make it stronger/more dense, we put force to the bone)
C.1.4 Discuss how studies of different populations provide evidence of the link between physical activity and hypokinetic disease
Various populations changed their lifestyles from one of high physical activity (traditional, agricultural-based living) to one of low physical activity ("westernized living")
CHD and stroke account for a large % of deaths in high income countries
In the past we had more movement but now we sit more
C.1.5 Discuss the relationship between major societal changes and hypokinetic disease
Examples of changes:
->Include the proliferation of the motor vehicle
-> Changes in employment and working patterns
->Changes in the diet such as the raise of fast food
C.2 Cardiovascular disease (CVD)
term given to classify a group of disorders of the heart and blood vessels. (mainly consists of hypertension/high blood pressure, coronary heart disease and stroke)
A major cause of CHD and stroke (and define)
ATHEROSCLEROSIS: hardening of the arteries due to the accumulation plaque (made up of cholesterol and other substances) in the walls of arteries.
->pieces of plague can break arteries
->If a block occurs in a coronary circulation (blood supply -> heart) this leads to heart attack!
->If the blockage occurs in a blood vessel in the brain -> Stroke!
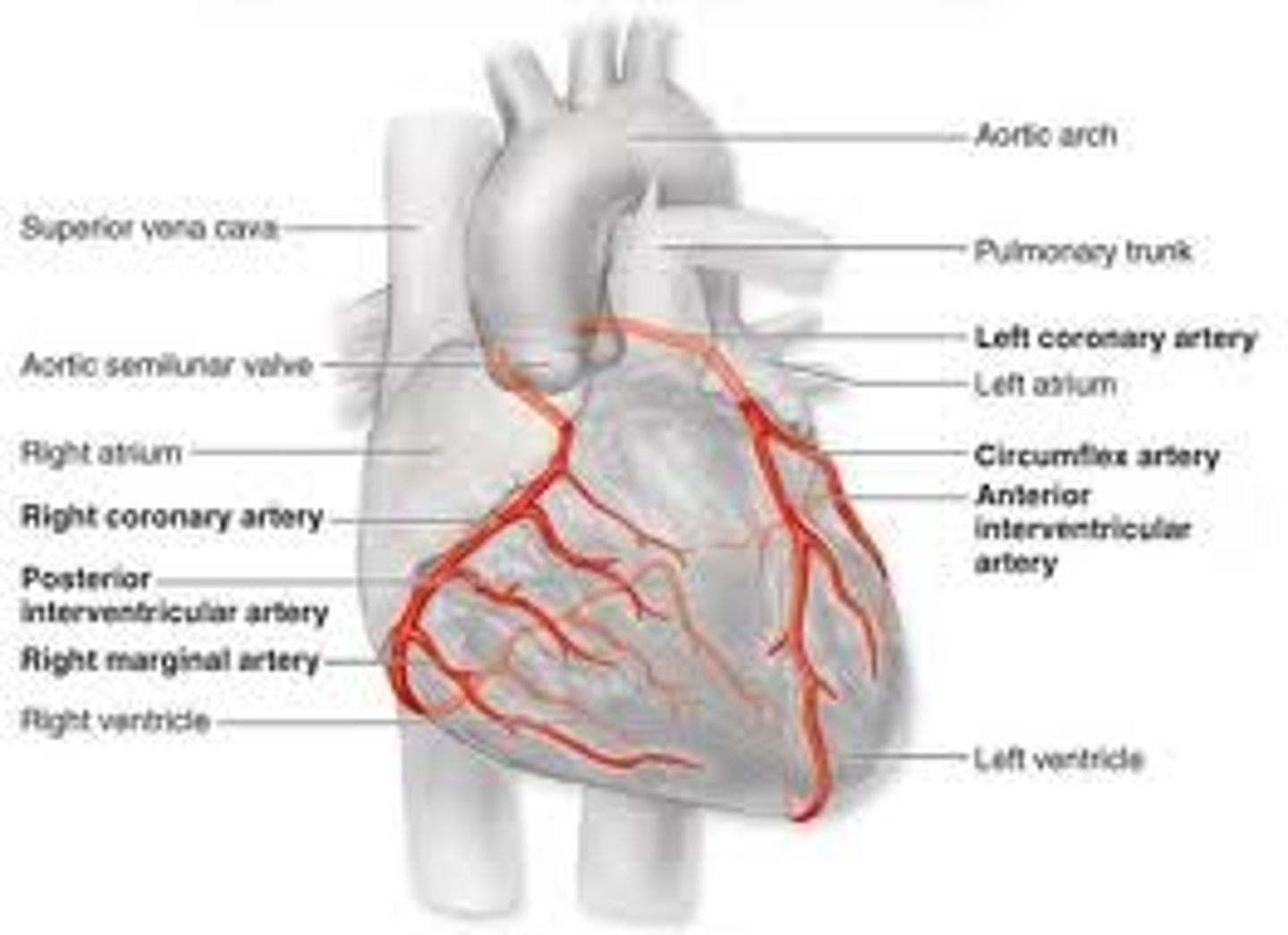
C.2.1 Outline the coronary circulation
coronary circulation: how blood transfers through heart & how blood supplies itself
->Left and right coronary arteries
->circumflex artery
->left anterior descending artery
(image shows it)
C.2.2 Outline what is meant by the term atherosclerosis
ATHEROSCLEROSIS: hardening of the arteries due to the accumulation of plaque (made up of cholesterol and other substances) in the walls of arteries = blood clot
C.2.3 List the major risk factors for cardiovascular disease
-> MODIFIABLE (influenced by lifestyle; can change) - physical inactivity one of the major factors
-> cigarette smoking
-> hight blood pressure (hypertension)
-> High cholesterol and LDL-cholersterol
-> Low HDL cholesterol
-> Diabetes
-> Obesity
->Physical Inactivity
-> NON-MODIFIABLE (can't change)
->Age
-> Gender
-> Ethnicity
->Family History
HDL Cholesterol
plays an important role in removing excess cholesterol from the body in a process termed " reverse cholesterol transport"
->insoluble, carried with the bloodstream in lipoproteins
Different relationship with CVD
-> (LDL) low density lipoprotein (increases the risks of CVD)
-> (HDL) hight density lipoprotein (decreases the risks of CVD)
exercise raises HDL cholesterol concentrations
C.2.4 Explain the concept of risk factors in cardiovascular disease
Factors can group together, forming what's termed metabolic syndrome when three or more factors cluster. Key components include high triglycerides (blood fat) and low levels of HDL-cholesterol, impaired glucose regulation or diabetes, especially abdominal obesity. This clustering heightens the risk of cardiovascular disease (CVD).
Show Exercise may lower the risk of CHD (4 reasons)
-> may have direct effects on the heart;
increasing the size of the coronary arteries and making them less likely to get blocked
-> improves endothelial function which means that arteries are able to vasodilate (open up) on demand to increase blood supply, reduce the chances of ischemia
->helps to prevent obesity thus reducing the risk of blood clots forming
->major positive effect of exercise is helping to maintain high levels of protective high density cholesterol (HDL)
C.2.5 Discuss how a lifestyle of physical inactivity increases the risk of cardiovascular disease
People who are physically inactive are more likely to have risk factors for CHD, high blood pressure, obesity, type 2 diabetes, low HDL Cholesterol --> increases risk of CHD
C.3.1 Describe how obesity is determined (along with limitations on calculations and effects on childhood obesity)
Obesity is by definition an excess of body fat, but in reality it is determined using indirect measurements of body, for example body fat index BMI and waist circumference
BMI a measurements of body fat, calculated by dividing weight in kilograms by height in meters squared - > indirect assessment of body fat percentage (inits kg/m^2)
A BMI less than 18.5= under
A BMI between 18.5 and 25= normal
A BMI between 25-30= overweight (Obese I)
A BMI 30-40 = obese (Obese II)
A BMI 40+ = morbid obese (Obese III)
Values can be often misleading - bodybuilders weightlifters, large muscles
Childhood obesity-> associated with social stigmatization and bullying (This raises an ethical issue around the routine)
More accurate assessments of body fat %s: (and their limitations!)
-> sophisticated imaging techniques, including dual energy x-ray absrptionmetry (DXA), magnetic resonance techniques (MRI), and computed tomography (CT)
-> can be costly
->time consuming, DXA/CT low doses of radiation
C.3.2 Outline the major health consequences of obesity
->Cardiovascular disease and hypertension
->type 2 diabetes
->osteoarthritis
->respiratory problems
->some forms of cancer
C.3.3 Discuss the concept of energy balance
Energy Balance is affected mainly by food intake, resting metabolic rate and physical activity.
(balance occurs when input = output)
It is determined by energy intake and energy
expenditure as follows:
-> Energy intake > energy expenditure = weight gain
-> Energy intake < energy expenditure = weight loss
-> Energy intake = energy expenditure = stable body weight
C.3.4 Outline how chemical signals arising from the gut and from the adipose tissue affect appetite regulation
-> Hormones are produced by the stomach and small intestine after eating and by adipose tissue (leptin). These pass to an appetite control centre in the brain (hypothalamus) that regulates feelings of hunger and satiety.
->regulate appetite GHRELIN, LEPTIN (supresses appetite, obese ppl deficient in this = always hungry)
-> exercise helps to reduce both subcutaneous fat ( underneath the skin and the fat within the abdomen)
C.4 Physical activity and type 2 diabetes
elevated glucose concentrations,hyperglycemia (may be elevated
(glucose stores energy)adipose tissue cells move glucose from blood to liver and muscle
C.4.1 Compare type 1 and type 2 diabetes
both can cause death or hyperglycemia
C.4.1 Contrast TYPE 1 Diabetes:
TYPE 1: (do not produce insulin) is an autoimmune disorder resulting in the destruction of the insulin-producing cells of the pancreas. It usually manifests in young people.
(can be treated with insulin)
Contrast TYPE 2 Diabetes:
is a disease of insulin resistance, particularly in skeletal muscle and is highly related to obesity and older age / family history
(can be treated with exercise and diet/oral medication/ insulin)
C.4.2 Discuss the major risk factors for type 2 diabetes
obesity, family history, diet, physical inactivity
C.4.3 outline the health risks of diabetes
-> blindness (retriopathy)
-> kidney disease
->nerve damage
-> cardiovascular disease (stroke)
Adult Onset Diabetes
emerged in children - environmental factors - poor diet , - low levels of physical activity
C.5.1 Outline how bone density changes from birth to old age
Bone mass density increases from birth through to around 35-45 years of age. Typically females achieve a lower-peak bone density than males. From this age onwards, bone mass density decreases (esp in women post menopause)
C.5.2 Describe the risk of osteoporosis in males and females
low bone mineral density can lead to osteoporosis which leaves a person more vulnerable to fracturing bones-> mostly females post menopause
2 factors determine whether or not a person develops osteoporosis:
->Their peak bone mass as a young adult
->The rate of bone loss with aging
exercise can affect both of these factors
C.5.3 Outline the longer-term consequences of osteoporosis in males and females
-> independence
-> development of secondary complications as a result of long-term hospitalization and pneumonia
-> fragile bones
C.5.4 Discuss the major risk factors for osteoporosis
-> lack of dietary calcium
-> cigarette smoking
-> slim build ectomorphy
-> lack of estrogen associated with early menopause and female triad
-> physical inactivity
->excessive exercise in females who keep their body mass low
C.5.5 Discuss the relationship between physical activity and bone health
- Weight-bearing physical activity is crucial for bone health, but intense training in weight-conscious athletes can lead to low body weight and eating disorders, causing menstrual dysfunction and osteoporosis.
- Bone density changes vary by site, with resistance training having a greater impact than endurance training.
- Childhood is critical for optimizing bone health through weight-bearing exercise, as failure to do so increases the risk of osteoporosis later in life.
C.6.1 Outline physical activity guidelines for the promotion of good health
150 minutes a week of moderate intensity exercise
75 minutes of high intensity exercise
For people 18-64
Prevents osheimeres
C.6.2 Describe the aims of exercise in individuals with a hypo kinetic disease
->to make the most of limited functional capacities
-> to alleviate or provide relief from symptoms
-> to reduce the need for medication
-> to reduce the risk of disease recurrence
-> to help overcome social problems and psychological distress
C.6.3 Discuss the potential barriers to physical activity
-> Physical ( perceptions of being to old or too fat
-> Emotional ( shyness, embarrassment)
->Motivational (lack of energy for or enjoyment of exercise )
->Time ( lack of time due to work or family life)
->Availability (perceptions, lack of equipment, facilities and the feeling that there is no one to exercise with)
- uncontrolled disease state (unstable angina, poorly
-controlled diabetes, uncontrolled hypertension)
- hazards of exercise
-musco-skeletal injuries
-triggering of other health issues (heart attack, respiratory tract infections)
C.7.1 Define the term mood
temporary emotional state
C.7.3 Outline how exercise enhances psychological well-being
PSYCHOLOGICAL:
distraction from daily hassles and routine
enhanced feeling of control
feeling of competency
Positive mood, social interactions
Improved self-concept and self-esteem
->refers to a set of feelings experienced on a day-to-day basis.
->mood states can last for hours, days, weeks, or even months
->distinct from emotions - lasts longer, emotions are feelings generated in response to specific events, lasting for minutes, hours
->Can be positive (happiness, vigour) and negative (anger, anxiety, depression, fatigue)
C.7.2 Outline the effects of exercise on changing moods states
Exercise helps improve mood reducing fatigue, anger, anxiety, and depression, while also boosting energy, clarity of thought, and sleep quality.
It enhances overall well-being, self-esteem, and can positively impact women's experiences during menstruation, pregnancy, and menopause.
These benefits, attributed to increased levels of endorphins, norepinephrine (which improves circulation), and serotonin (leading to reduced depression and anxiety)
seen in both healthy individuals and those with diseases or disabilities.
C.7.4 Explain the role of exercise in reducing the effects of anxiety and depression
exercise can be used as treatment
nature of the exercise programme (enjoyable, aerobic, rhythmic, absence of interpersonal competition, closed and predictable environment)
20-30 minutes, several times per week
stress relief
C.7.5 Discuss the potential personal and environmental barriers to physical activity
ENVIROMENTAL:
Social environment (feelings that there is no one to exercise with)
Physical environment (perceptions of being too old or too fat)
Characteristics of physical activity (lack of enjoyment of a particular exercise)
Social and cultural norms
Depression
sad mood, lack of interest, guilt, sleep/appetite changes, low energy, poor focus. It can harm daily life, lead to suicide
C.7.6 Describe strategies for enhancing adherence to exercise
Environmental approaches - prompts, contracting, perceived choice
Reinforcement approaches - rewards for attendance and participation, external feedback, self-monitoring)
Goal Setting - associative vs. dissociative focus during exercise
Social support - role of others (spouse, family members, friends), including joining in, adjusting routines, transportation, providing equipment
C.7.7 Outline the possible negative aspects of exercise adherence
negative addiction - life choices and relationship issues --> can cause death or cardio/resp. problems
increased tolerance to exercise, subjective awareness of compulsion to exercise
adverse mood states with withdrawal