


Chapter 32: Corrosive Poisons
32.1: Corrosive Poison
Corrosive poisons are those substances, which corrode (means –‘to eat away’) and destroy tissues through direct chemical action.
They can be classified into two groups:
Strong Acids
Inorganic acids (mineral acids): Sulfuric, nitric, hydrochloric and hydrofluoric acids.
Organic acids: Carbolic, oxalic and salicylic acids. These acids are weaker in action compared to inorganic acids and are usually absorbed into circulation, promoting local and remote action.
Strong Alkalies
Anhydrous ammonia
Potassium hydroxide
Sodium hydroxide
Ammonium carbonate
Potassium carbonate
Sodium carbonate
32.2: Inorganic Acids
Only strong acids and alkalies act as corrosives.
Dilute acids and alkalies act as irritants.
Strong acids produce coagulation necrosis characterized by the formation of a coagulum as a result of the desiccating action of the acid on proteins in superficial tissues.
The coagulum formed limits the penetrating ability of acids.
Strong alkalies create injury to tissue by the mechanism of liquefaction necrosis.
Alkalies, unlike acids, produce extensive penetrating damage.
Squamous epithelium of esophagus is more resistant to acids than columnar epithelium of stomach.
Squamous epithelium of the esophagus is more sensitive to alkalies than columnar epithelium of the stomach.
Esophageal strictures are more common in alkali poisoning and pyloric and gastric strictures are more common in acid poisoning.
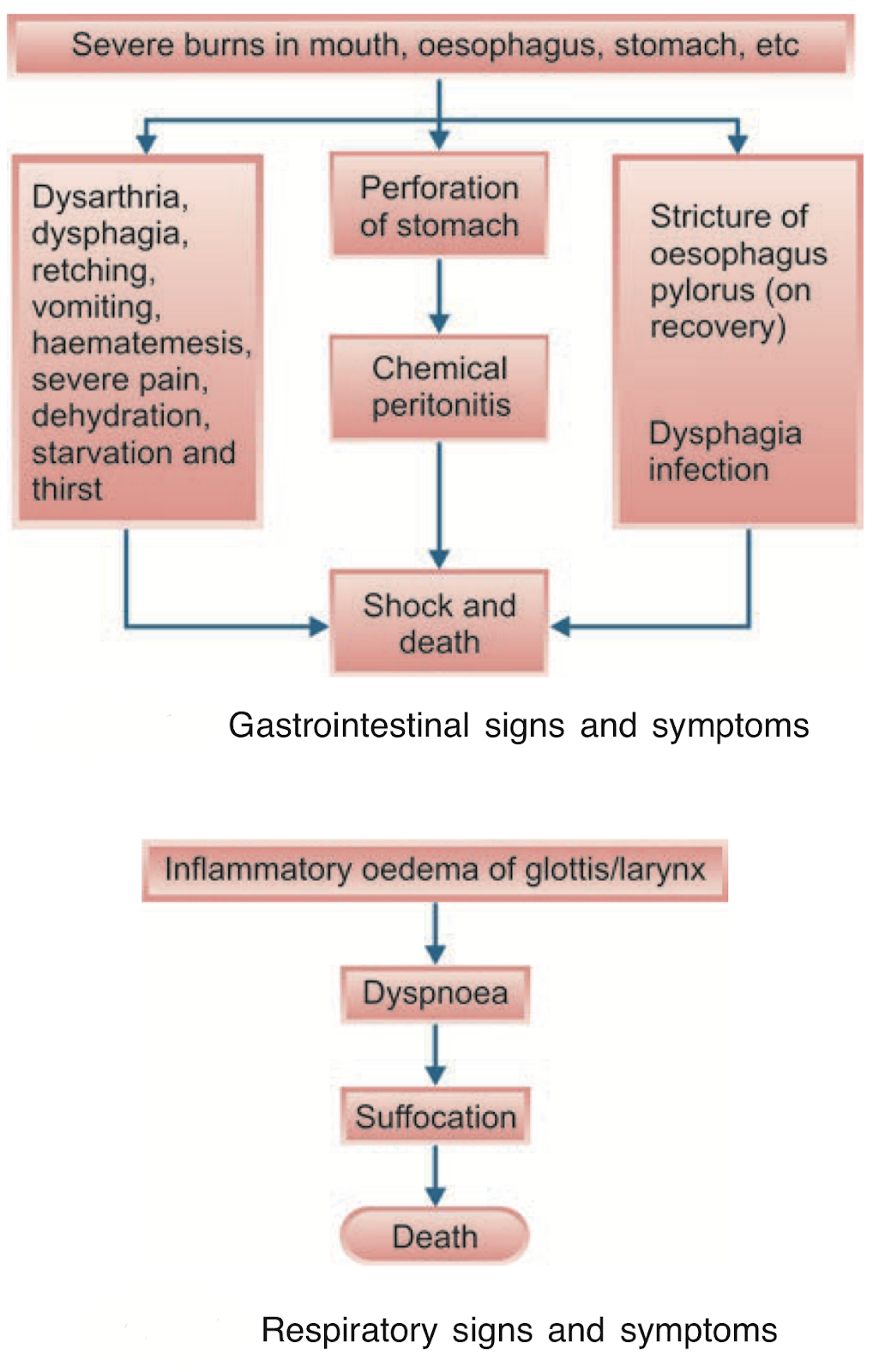
Signs and Symptoms
Treatment
Avoid
Gastric lavage as to prevent gastric perforation (exception: organic acids).
Administering carbonates, which can yield CO2, producing distention and perforation.
Emesis is not attempted for fear of rupture of the stomach.
Give
Milk (canned condensed milk), egg white (beaten), vegetable oils, starch solution, barley water, thin gruel, etc.
Immediate dilution with milk or water within 30 minutes post ingestion is widely recommended for oral ingestions despite the fact that tissue injury occurs rapidly.
Airway maintenance and artificial respiration if there is any respiratory distress.
Morphine/pethidine for relief of pain.
Intravenous fluids and electrolytes for dehydration.
No oral feed until endoscopy confirms the extent of injury.
Antibiotics for control of infections.
Corticosteroids have proved to be good in delaying or preventing stricture formation in experimental animal studies; there is a controversy in recommending it for human beings.
Skin care for any skin lesions involves copious saline irrigation.
Treat with non adherent gauze and wrapping.
Eye care for any acid injuries to the eyes requires copious irrigation with retraction of eyelids for 20-30 minutes.
Antibiotic eye drops can help combat infections.
Causes of Death
Causes of death could be immediate or delayed
Immediate causes are suffocation and asphyxia due to edema of glottis; exhaustion; and shock due to circulatory collapse or perforation of stomach, while delayed causes are starvation and dehydration due to stricture of esophagus or pylorus.
The victim may also die due to peritonitis or secondary infections.
Postmortem Findings
Corrosion of parts that come in contact with it especially lips, mouth, throat, chin, angle of mouth, hands, etc. and also clothing, furniture, etc. when spilled over them.
The findings are restricted to the upper gastrointestinal and respiratory tract, and they are:
Pharynx and esophagus: Inflammatory changes with edema and bleeding.
Stomach: It is converted into a soft, boggy black/yellowish/brownish, which disintegrates on touch.
Surrounding viscera: Sloughing is seen if stomach wall is perforated. Perforation is most common in case of sulfuric acid.
Larynx and trachea: These show corrosion and inflammation. Congestion of the respiratory tract is commonest in case of nitric acid poisoning due to inhalation of acid fumes.
Chemical Tests
Sulfuric acid: With barium chloride or nitrate, it produces white precipitate of barium sulfate.
Nitric acid: Nitric Acid when added by the side of a test tube containing a mixture of ferrous sulfate and sulfuric acid, a brown ring appears at the interphase.
Hydrochloric acid: When mixed with silver nitrate, it produces a curdy white precipitate of silver chloride.
Medicolegal Importance
Sulfuric acid is often mistaken for glycerine or castor oil and consumed.
Rarely used for committing suicide.
Extremely rare in committing homicide.
Occasionally used as an abortifacient.
Vitriolage: Death or disfiguration due to throwing of concentrated sulfuric acid on the face of a person with an intention to produce damage.
Xanthoproteic reaction: It is a local reaction producing yellowish discoloration of the tissues upon contact with concentrated nitric acid.
Attempts of disposal of dead body after killing has been reported in history.
32.3: Hydrofluoric Acid
Hydrofluoric acid is a colorless gas, which becomes a fuming liquid when dissolved in water and is used for etching glass and clouding electric bulbs.
Fatal dose: 15mL.
Fatal Period: Few minutes to 2 hours.
The fluoride anion produces a liquefaction necrosis by binding with calcium and magnesium in the tissues.
This also results in hypocalcemia, rendering hydrofluoric acid poisoning more serious.
Following ingestion, patient presents with hematemesis, hypovolemic etanic convulsions, upper airway obstruction, severe hypocalcemia, acidosis, shock and coma.
Myocardial irritability and subsequent life-threatening cardiac arrhythmias may be due to binding of potassium, magnesium and calcium ions.
Skin exposure can result in severe and deep burns, which are extremely painful and slow to heal.
Treatment
Acid burn lesions need copious irrigation with water, application of calcium gluconate gel, and debridement if needed.
Intra-arterial infusion of 20 percent calcium gluconate or calcium chloride is effective.
Oxygen inhalation after removal from fumes and tracheotomy, if needed, should be done.
Postmortem Findings
Lips, tongue, and mouth may show white patches or maybe charred esophagus may show shredded epithelium with ecchymosis, inflammation, ulceration, and blackening of the stomach.
Liver and kidneys show fatty and parenchymatous degeneration.
32.4: Carbolic Acid (Phenol)
Carbolic Acid — It is a poison that can be identified by smell, which is commonly referred to as phenolic odor or hospital odor.
Pure phenol has a colorless, short, prismatic needle-shaped crystalline form.
On exposure to air, it turns pink and liquefies. It is fat-soluble, hence can attack the nervous system.
It is also soluble in glycerin, ether, alcohol and slightly in water.
It is known specifically for its antiseptic or disinfectant property.
Phenol is a protoplasmic poison. It enters into a loose combination with proteins and penetrates deep into the tissue.
When applied to skin or mucosa, it causes necrosis and gangrene.
The local nerve endings are first stimulated and then paralyzed, resulting in anesthesia.
After absorption, it causes widespread capillary damage and clotting in superficial blood vessels.
It also acts on the cells of central nervous system, heart and kidneys.
Phenol is metabolized mainly by the kidneys, wherein it gets converted into hydroquinone and pyrocatechol and excreted in urine (both).
These products turn urine olive green or brown on standing, and the phenomenon is called carboluria.
Complete elimination occurs in 36 hours.
Phenol is considered as a nephrotoxic drug. Other nephrotoxics comprise heavy metals, methanol, oxalic acid, salicylates, phenacetin, EDTA and penicillamine.
Other Members of Phenol Group
Cresol: A methyl phenol with meta, ortho and para isomers. It is used as a disinfectant and antiseptic.
Creosote: A mixture of phenols and consists mainly of cresol and guiacol. It is used as a household remedy for coughs and is found in many proprietary preparations.
Resorcinol: A colourless crystalline substance and is used for the treatment of various skin diseases including ringworm, psoriasis, eczema, etc.
Lysol: 50% solution of cresol (3-methyl phenol) in saponified vegetable oil.
Dettol: Chlorinated phenol, parachlorometaxylenol and is practically non-toxic to adults.
Thymol: An alkyl derivative of phenol obtained from volatile oils of Thymus vulgaris, Monarda punctata or Trachyspermum ammi.
It occurs in colorless crystals with characteristic pungent odour and taste.
It was used earlier as an antihelminthic (for ankylostomiasis), antifungal and antiseptic.
Signs and Symptoms
The usual signs and symptoms of carbolism are:
Headache, giddiness, tinitus
Vomiting, diarrhea and pain abdomen
Muscular spasms and convulsions
Collapse—unconsciousness, coma
Clammy, cold, sweating body
Stertorous breathing with cyanosis
Pupils dilated
If survives for 48 hr—carboluria followed by anuria. Victim will pass dark, smoky urine which soon turns olive green on standing.
Methemoglobinaemia is a characteristic feature in severe cases.
Death may result from respiratory and circulatory failure.
Treatment
In case of poisoning through skin absorption, perform the following:
Remove the contaminated garments
Cleanse the site by mopping with wet cloth and wash with soap and water.
Apply olive oil/ methylated spirit/ 10 per cent ethyl alcohol, which can prevent further absorption
Shift the victim to fresh atmosphere and make him breath in fresh air
Give normal saline + sodium bicarbonate (I/V- drip).
In case of poisoning through oral route, perform the following:
Perform gastric lavage: Though phenol corrodes the stomach wall, it also hardens it unlike other corrosive poisons.
Gastric lavage is performed whenever possible with plenty of lukewarm water containing animal charcoal, olive oil, magnesium or sodium sulfate or saccharated lime, soap solution, 10 percent glycerine, etc.
When the lavage is completed, 30 gm of magnesium sulfate or medicinal liquid paraffin should be left in the stomach.
Give egg white: Epsom salt/demulcents orally.
Symptomatic:
Artificial respiration.
Tracheal aspiration of froth/secretions.
Glucose saline to induce diuresis.
Postmortem Findings
External: No specific findings. However, burns of the face and skin rarely seen.
Internal: Mucosa of the mouth, tongue, pharynx and esophagus are bleached (whitened/scald/red), if a strong solution is consumed.
Stomach changes:
The stomach mucosa is reddened and punctate due to erosions giving “velvety red” or blackish appearance
Wall of the stomach is softened, but no perforations
Contents: Gelatinous brown (due to acid hematin formation).
Kidney changes:
Swollen and congested.
Tubules on histopathological study reveal to be filled with oxalate crystals.
Medicolegal Importance
Usually consumed accidentally (mistaken for magnesium sulfate)
Suicidal or homicidal uses are rare due to the taste
As an abortifacient: occasionally used to induce criminal abortion
Used for illegal erasure of signatures
It is detected in certain vegetables as oxalate, e.g. beets and in the leaves of spinach, rhubarb, cabbage, etc and many other vegetables.
Commercial uses:
Cleaning or bleaching leather
Book binding
Calico printing
Removal of iron molds from linen
Removal of the ink stains.
32.5: Formic Acid (Methanoic Acid)
Formic acid is a colorless liquid with a pungent penetrating odor, completely soluble in water.
Formic acid is unique for its ability in many patients to cause death after a prolonged (several weeks) course of classical acid-induced gastrointestinal damage.
Certain other complications include severe metabolic acidosis, intravascular hemolysis, and disseminated intravascular coagulation.
Accidental ingestion in children ordinarily does not lead to fatalities, since the pungent taste prevents ingestion of a lethal dose.
It is nevertheless a problem when used deliberately for suicide.
It causes acute tracheobronchitis, characterized by cough, sore throat, chest pain and light-headedness.
Formic acid skin burns may also result in systemic toxicity.
When absorbed by the body, it causes systemic acidosis, hematuria and renal damage. Metabolism of methanol can also produce toxic metabolites of formic acid.
Treatment is by correction of acidosis by infusion of sodium bicarbonate intravenously and to treat renal failure by hemodialysis.
32.6: Strong Alkalies
Alkalies generally contain hydroxyl groups, which on dissociation in water produce hydroxide ions.
Alkali agents create injury to the gastrointestinal tract by the mechanism of liquefaction necrosis, whereby saponification of fats and solubilization of proteins allow deep penetration into tissue.
It produces extensive penetrating damage. This pathogenesis of injury is rapidly progressive, and may extend to weeks after onset.
Alkalies cause more severe corrosive effects on the esophagus, than on the stomach, as in the case with acids.
Severe esophageal damage can occur, if the pH is lower than 11.
32.7: Anhydrous Ammonia
Ammonia is an irritant gas. It is highly soluble in water.
Gaseous ammonia when dissolved in water forms a strong solution of ammonia known as Spirits of Hartshorn, which contains 32.5% of ammonia and is a colorless pungent liquid used in agriculture, mining, plastic, and explosive industries.
It is absorbed into the respiratory tract and has its pulmonary effects, causing pulmonary edema and direct mucosal injury by alkaline burn.
Gaseous ammonia causes running nose and increased salivation. It can induce asthma, severe upper respiratory tract irritation, pneumonia, pulmonary edema, bronchitis, and obstructive lung disease.
Death is usually due to bronchopneumonia.
Ammonia ingested can produce intense pain, dysphagia followed by esophageal stenosis.
Exposures results in watering of the eyes, corneal damage, conjunctivitis and palpebral edema. Blindness may be a serious consequence in severe cases.
Fatal Dose:
Liquid form — 10-30mL.
Gaseous form — 0.5% in air.
Removal from exposure and rest, including symptomatic treatment; corneal irrigation with water and topical antibiotics, should be done.
32.8: Other Alkalies
Potassium Hydroxide and Sodium Hydroxide: These are used as drain and oven cleaners.
Fatal Dose — 5g.
Ammonium Carbonate: It is a translucent, hard crystalline mass with a strong ammoniacal taste and pungent odor.
Potassium and Sodium Carbonate: They are white crystalline powder and are very soluble in water, but not in alcohol. They are used for cleaning and washing purpose.
Fatal Dose — 15g.