


Human Physio Cardiovascular
Cardiovascular system
The Heart
muscular pump that drives flow of blood to various organs
Blood vessels
conduit through which the blood flows
Blood
fluid that circulates around the body
carrying materials to and from the cells
Blood flow through cardiovascular system
Arteries take blood away from heart.
Veins return blood to the heart.
Series flow: blood travels trhough systemic and pulmonary circuits in series
portal system: two capillary beds connected in series
Anatomy of the heart
Located in thoracic/chest cavity between the lungs
Pericardium - a double serous membrane
Visceral pericardium - next to heart
Parietal pericardium - outside layer
Serous fluid fills the space between the layers of pericardium
Heart wall
Composed of three distinct layers
Epicardium
connective tissue layer
same as visceral pericardium
Myocardium
cardiac muscle, thickest layer
Endocardium
endothelium
contains the Purkinje fibers

Heart chambers and Valves
Four chambers
Two atria receive blood returning to the heart from vasculature
Two ventricles receive blood from atria and push the blood out of heart
Heart valves
Promotes unidirectional blood flow
Atrioventricular (AV valves) - between atria & ventricles
Semilunar valves - between ventricles and arteries
Path of blood flow
Blood comes into the right atrium from the body
Moves into the right ventricle
Pushed into the pulmonary arteries in the lungs.
After picking up oxygen, the blood travels back to the heart through the pulmonary veins into the left atrium
Into to the left ventricle and
Out to the body's tissues through the aorta.
Electrical conduction in the heart
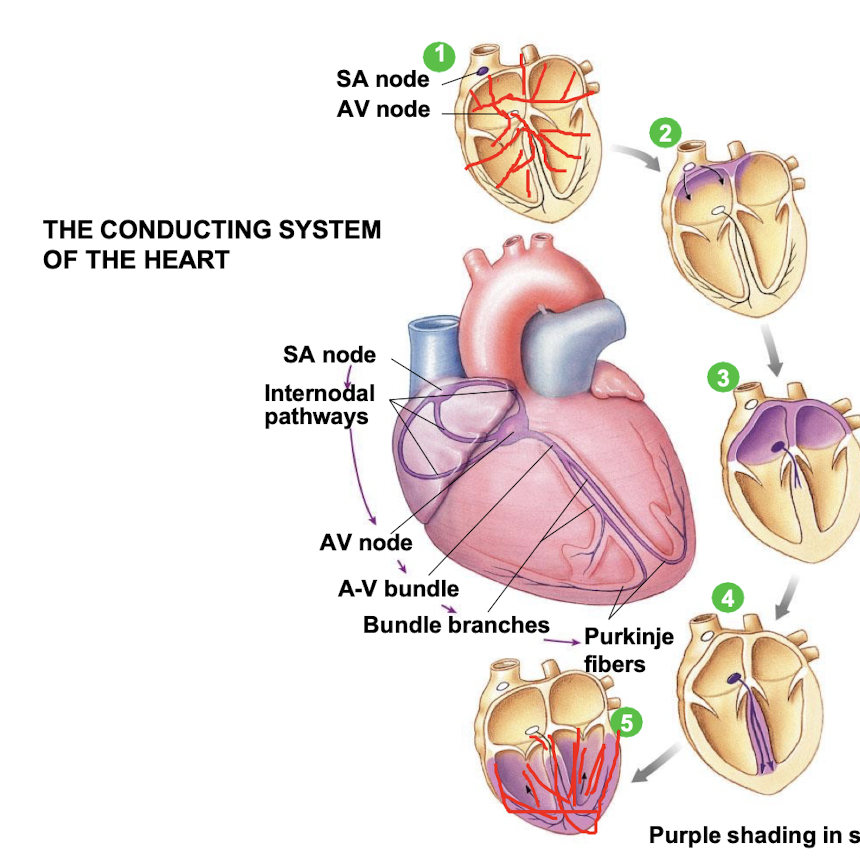
SA node depolarises
Electrical activity goes rapidly to AV node via internodal pathways
Depolarisation spreads more slowly across atria. Conduction slows through AV node.
Depolarisation moves rapidly through ventricular conducting system to the apex of the heart.
Depolarisation wave spreads upward from the apex.
Control of heart rate
Both SA node and AV node - capable of generating spontaneous action potentials
SA node usually sets the pace of heartbeat
fires more frequently than AV node (70 impulses/min compared to 50 impulses/min)
cells in AV node stimulated by impulses coming from SA node → go into refractory period
If SA node fails to fire or if impulses from it are blocked, the AV node can take over
Electrocardiogram (ECG)
P wave
Atrial depolarisation
QRS complex
Ventricular depolarisation and atrial repolarization
T wave
Ventricular repolarization

P-Q interval
conduction through AV node
Q-T interval
ventricular systole (contracting)
T-Q interval
ventricular diastole (relaxing)
R-R interval
one heart beat
Cardiac Cycle
Events associated with flow of blood through the heart during a single complete heartbeart
various phases in the pumping action of heart
periods of valves opening and closure
changes in atrial, ventricular and aortic pressire
changes in ventricular volume
two major heart sounds
Phases of cardiac cycle
The heart cycles between contraction (systole) and relaxation (diastole)

Late diastole - both sets of chambers are relaxed and ventricles fill passively.
Atrial systole - atrial contraction forces a small amount of additional blood into ventricles.
Isovolumic ventricular contraction - first phase of ventricular contraction pushes AV valves closed but does not create enough pressure to open semilunar valves.
Ventricular ejection - as ventricular pressure rises and exceeds pressure in the arteries, the semilunar valves open and blood is ejected
Isovolumic ventricular relaxation - as ventricles relax; pressure in ventricles falls, blood flows back into cusps of semilunar valves and snaps them closed.
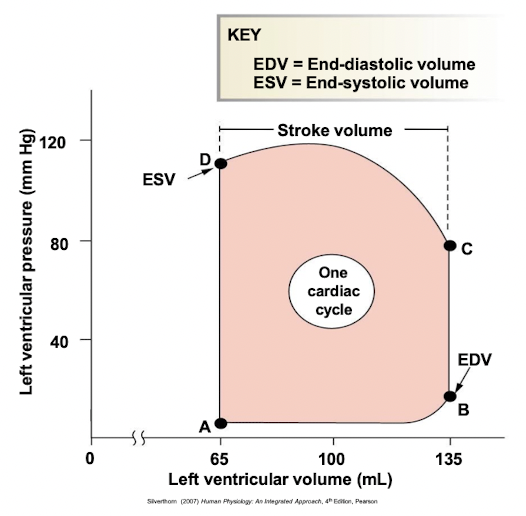
Pressure-volume curve
Left ventricular pressure-volume changes during one cardiac cycle
Stroke volume = EDV - ESV (70ml, at rest)
Cardiac output and control
Cardiac output (CO) = volume of blood pumped by one ventricle per minute
CO = HR x SV (heart rate x stroke volume)
Factors affecting cardiac output:
determined by heart rate, stroke volume or both
SV is directly correlated with CO, the greater the SV the greater the CO.
SV represents the difference in the amount of blood between: EDV and ESV
Control of stroke volume
Stroke volume (SV)
volume of blood pumped per ventricle per contraction
directly related to force generated by cardiac muscle during contraction
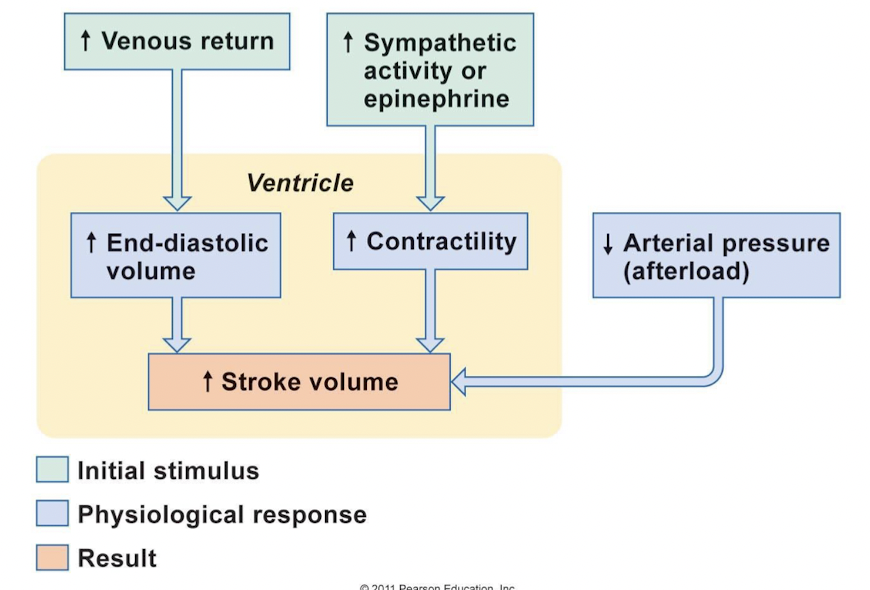
Primary factors affecting stroke volume:
end-diastolic volume (EDV)
ventricular contractility (force of contraction)
Preload (relate to EDV, degree of muscle stretch)
Afterload (pressure needed to eject blood out)
Ventricular contractility
Contractility
intrinsic ability of muscle fiber to contract at any given fiber length
function of Ca2+ interaction with contractile filaments
increase in contractility will increase stroke volume
Ionotropic agent
chemical that affects contractility → ionotropic effects
positive ionotropic effects - e.g. catacholamines (sympathetic stimulation) and drugs enhance contractility
End-diastolic volume (EDV)
volume of blood at the beginning of contraction (EDV) - determine the length of muscle
preload - degree of myocardial stretch before contraction begins
stretch of ventricular myocardium increases
SV increases (length-tension relationship)
Intrinsic control of cardiac function
Relationship between EDV and SV
Frak-Starling law of the heart
Frank-Starling law of the heart: Heart automatically adjusts its output to match EDV.
Increased EDV stretches muscle fibers.
fibers closer to optimum length
optimum length = greater strength of contraction
increased SV
Factors affecting EDV
primarily determined by end-diastolic pressure (preload)
preload increases, EDV increases and SV increases
preload affected by:
filling time - depends upon heart rate
atrial pressure - resulting from venous return and atrial contraction
factor influencing venous return is central venous pressure
central venous pressure rises, venous return increases, leads to increase in EDV
Summary of factors affecting stroke volume
Summary
Relate phases of ECG to events of cardiac cycle
Describe cardiac function and nervous system control of the heart
Describe blood flow, volume and pressure in relation to the control of cardiac function